

Abstract
Introduction: Persons with hemophilia A (PwHA) can develop pain resulting from joint and/or muscle bleeding over time, which can be debilitating and decrease quality of life. Hemophilia A guidelines recommend medications and other interventions to manage pain, however, little is known about how PwHA in the US use different interventions to manage pain. This study aims to describe interventions for pain management in PwHA in the US.
Methods: This retrospective cross-sectional analysis identified PwHA between 2006-2015 using data from Truven Health Analytics MarketScan® Commercial Database. PwHA were identified using a previously validated claims-based algorithm with high sensitivity and specificity (Lyons et al. Value Health 2018). PwHA with pain were identified if they had at least one medical claim for pain as identified by the International Classification of Diseases, Ninth and Tenth Revision codes (ICD-9 & ICD-10). Pharmacologic treatment alternatives, including prescription opioids, nonsteroidal anti-inflammatory drugs (NSAIDs), and adjuvant therapies(including antirheumatics, anticonvulsants, muscle relaxants, topical pain products, and corticosteroids), were identified using national drug codes from pharmacy claims and/or J-codes from medical claims. Non-pharmacologic physical therapy services, regardless of the reason for the procedure, were included and identified using common procedural terminology codes in medical claims. Data on over-the-counter pain medications were not available in the database and were not included in the study. Demographic and clinical characteristics of PwHA with evidence of pain were examined. Descriptive rates were reported for pharmacologic and non-pharmacologic pain interventions in PwHA with any pain and joint pain. Patterns of pain management by age subgroups were also described.
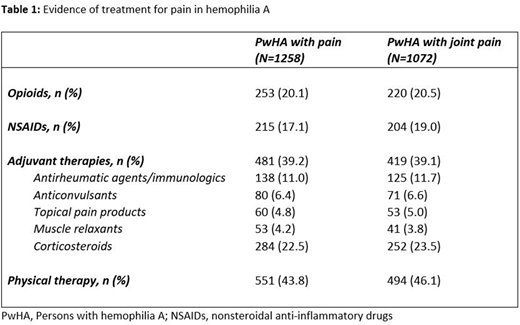
Results: We identified 2295 PwHA; of those, 1258 (54.8%) had evidence of any pain. The mean (standard deviation [SD]) age of PwHA was 21.9 (±15.3) years, with 99.7% males, mean (SD) Charlson Comorbidity Index (CCI) score of 0.27 (± 0.9); 44.9% had evidence of arthropathy, 8.9% of fracture, and 3.5% of joint replacement surgery. PwHA with evidence of pain were numerically older (23.4 ± 16.0 years), had higher mean CCI (0.32 ± 1.0) and a higher proportion of arthropathy (81.5%), fractures (14.5%), and joint replacement surgery (6.3%). Of the PwHA with evidence of any pain, 43.8% had at least one claim for physical therapy, 20.1% for prescription opioids, and 17.1% for NSAIDs. Similarly, physical therapy was the most common treatment recorded among patients with evidence of joint pain (46.1%), followed by prescription opioids (20.5%) and NSAIDs (19.0%). Approximately 39% of PwHA with evidence of any pain and joint pain received adjuvant therapies; however, the use of these agents cannot be completely attributed to pain management (Table 1). About a fifth of pediatric patients (<12 years) with any pain or joint pain had evidence of receiving prescription opioids (18.7% and 19.3%) and NSAIDs (6.9% and 8.2%), respectively, and these proportions increased with age. Among adults with evidence of any pain or joint pain, 25.1% and 26.1% of those in the age group of 45-64 years had received prescription opioids, and 26.8% and 28.8% had received NSAIDs, respectively.
Conclusions: Over half of the PwHA had evidence of any pain. Nearly half of PwHA with pain received physical therapy services for any reason, while approximately a fifth of PwHA with pain received prescription opioids and NSAIDs. These findings suggest a high prevalence of pain and pain management interventions in hemophilia A.
Raimundo:Genentech Inc: Employment, Other: Ownership interests PLC. Patel:Genentech Inc: Employment. Ko:F. Hoffmann-La Roche Ltd: Other: Ownership interests non-PLC; Genentech Inc: Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal